GENERAL MEDICINE CASE DISCUSSION
45 years old female with Paraparesis secondary to trauma a/w dysphagia since 15days.
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
CASE:-
HOPI:
Pt was apparently asymptomatic till 1999 then she delivered a baby(by c-section due to cord entanglement) she also stated that she started developed Generalized weakness ( due to low haemoglobin levels ) not associated with pain and was able to perform her daily activities
Her husband also left as she couldn't perform her daily activities.Her son currently stays in the hostel
She previously used to work as mandal officer.
And in 2012 she stopped going to work because she started developing weakness insidious in onset , gradually progressive , associated with pain , Aggrevated with walking and relieved with rest. she could not walk for long distances and she managed to to perform daily activities
In 2023 Jan she alleged had h/o slippage in bathroom following which she was normal for 5 days
Next day she couldn't get up from bed which is sudden in onset and non progressive and couldn't be able to perform her daily activities because of pain mainly and weakness of both the lower limbs.
Patient was taken to the nearby hospital and
X ray was done which is told to benormal
MRI was also done
Patient then complained of anuria for which foleys catherisation was done the she was able to pass urine
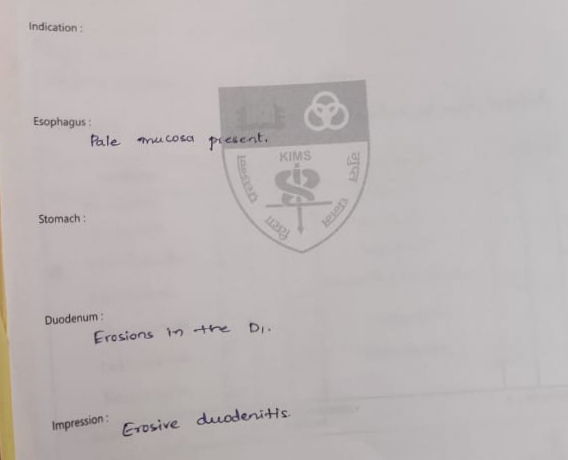
After 10 days she then developed difficulty in swallowing (more to solids ) associated with pain
No h/o giddiness,LOC, head injury
No history of involuntary movements
PAST HISTORY
N/k/c/o DM, HTN, thyroid disorders, CVA ,CAD, TB ,EPILEPSY
PERSONAL HISTORY
Diet: mixed
Appettite: decreased
Bowel and Bladder: regular
Sleep: adequate
No addictions
1/6/23
DAILY ROUTINE:
She is a Mandala Officer
She daily wakes at 6 Am and takes bath and fresh up drinks tea at 7am and then she takes her breakfast (RICE with vegetable curry )at 8am and goes for her mandala office and comes at 1 pm and takes her lunch which consisting of a vegetable curry and rice and after his lich he chit chat with her neighbors and lie down for some time and after that she watch TV and then eats her dinner at 8pm and goes to sleep at 9pm.
GENERAL EXAMINATION:
Patient is consious, coherent, and cooperative
moderately built and moderately nourished
Butterfly like rash present over the cheeks since 6yrs.









vitals
Temperature - AfebrilePulse - 83bpm
Blood pressure- 130/80 mmhg
Respiratory rate- 17 cycles per min
Spo2 - 99%

SYSTEMIC EXAMINATION
Power:-
Rt UL - 5/5
Lt UL-5/5
Rt LL - 2/5
Lt LL-2/5
Tone:-
Rt UL - normal
Lt LL- normal
Rt LL- normal
Lt LL- normal
Reflexes:
Right Left
Biceps: +++ +++
Triceps: ++ ++
Supinator: + +
Knee: - -
Ankle: - -
Plantar: Flexion. Flexion
Involuntary movements - absent
Fasciculations - absent
CVS :-
s1s2 heard,no murmurs
RS:-
Bae+,nvbs heard
P/A:-
soft,non tender,no organomegaly
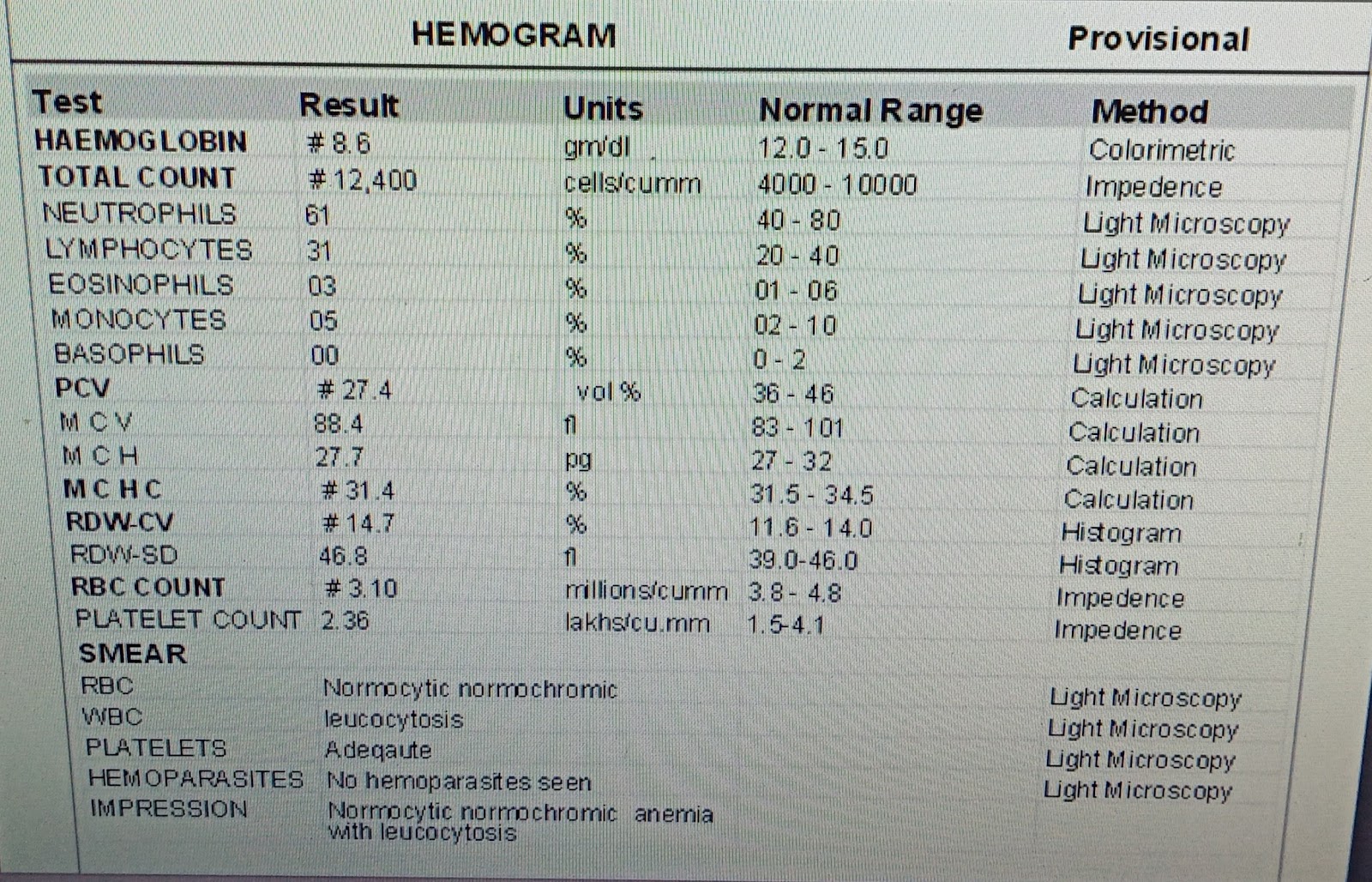
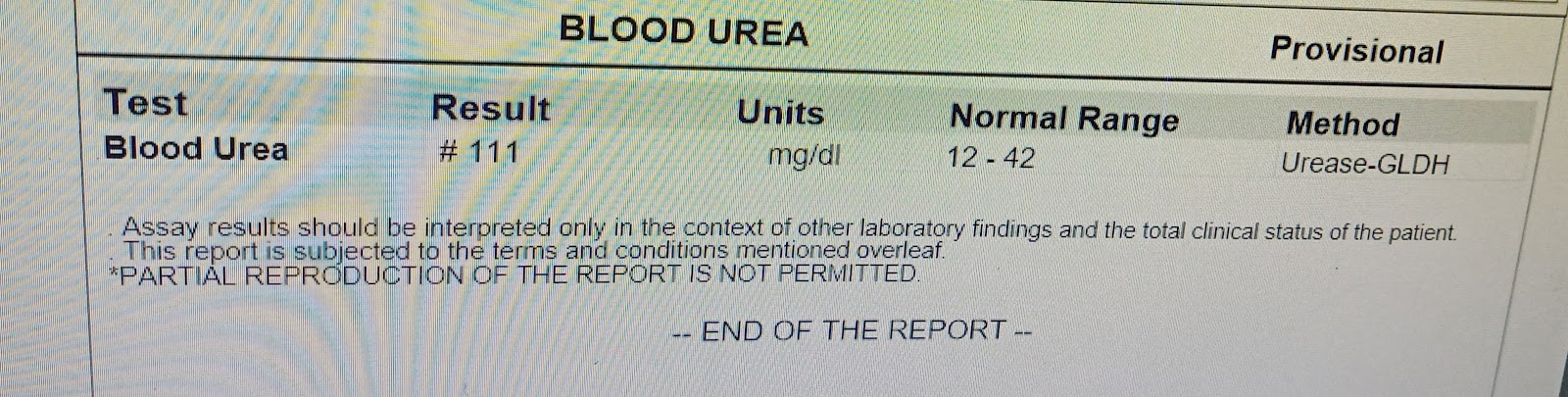
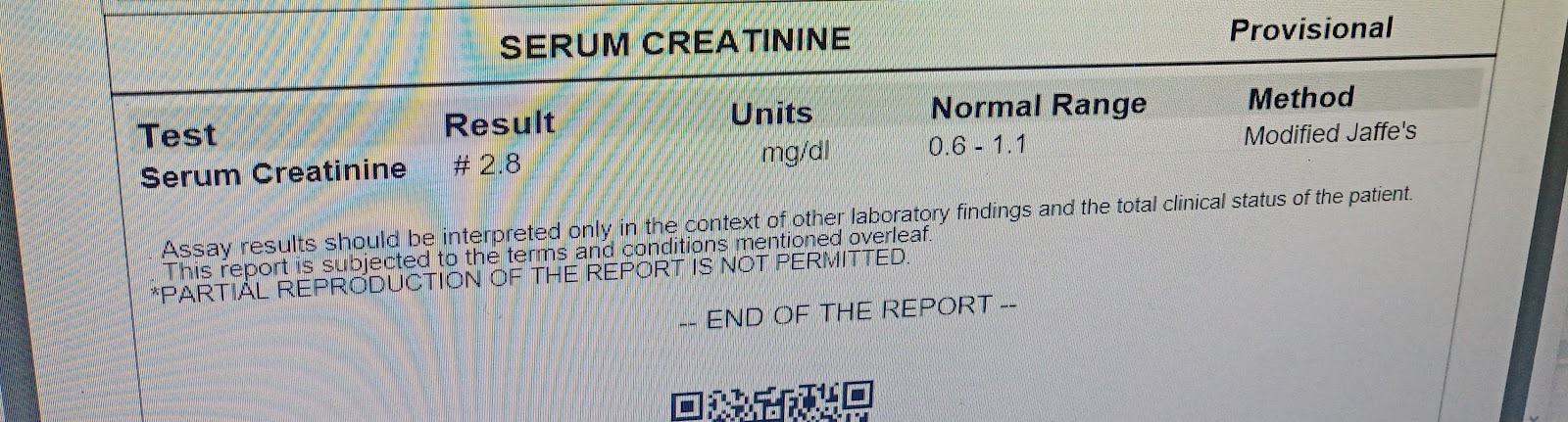
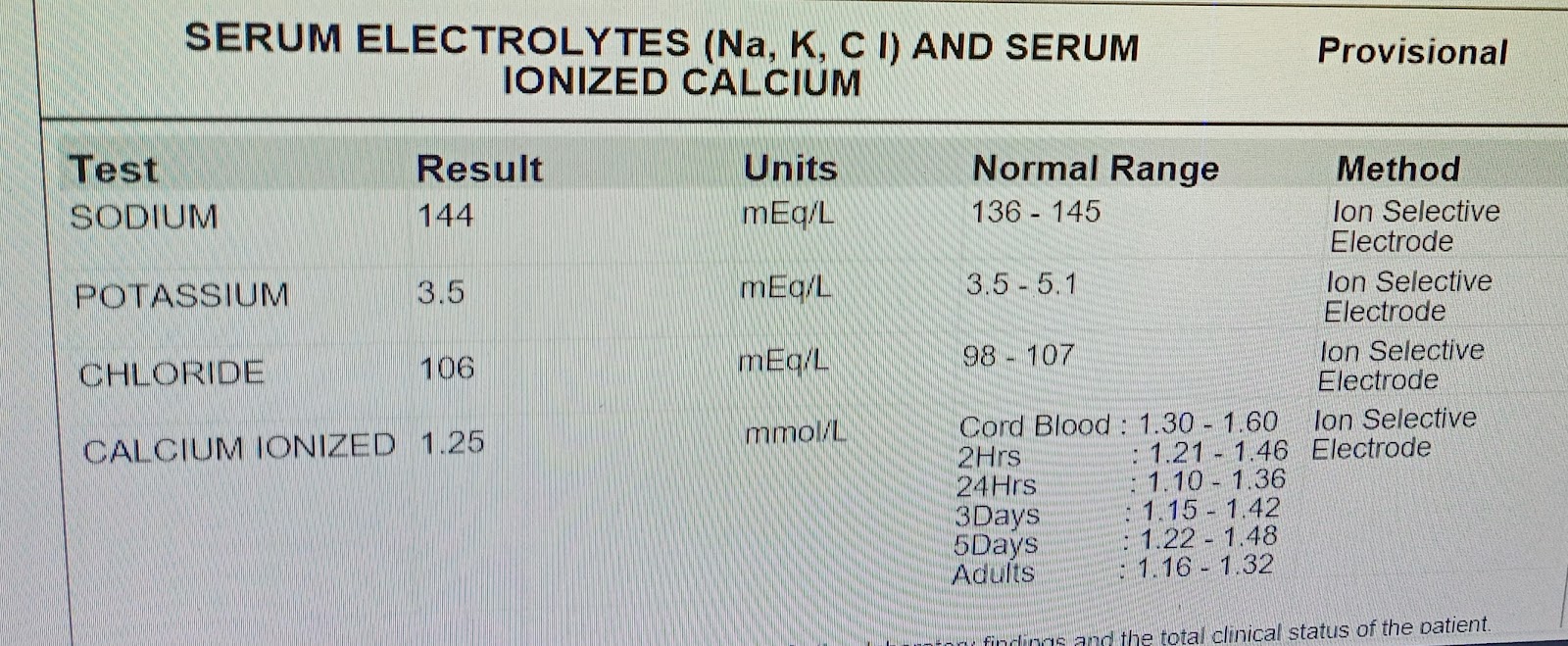
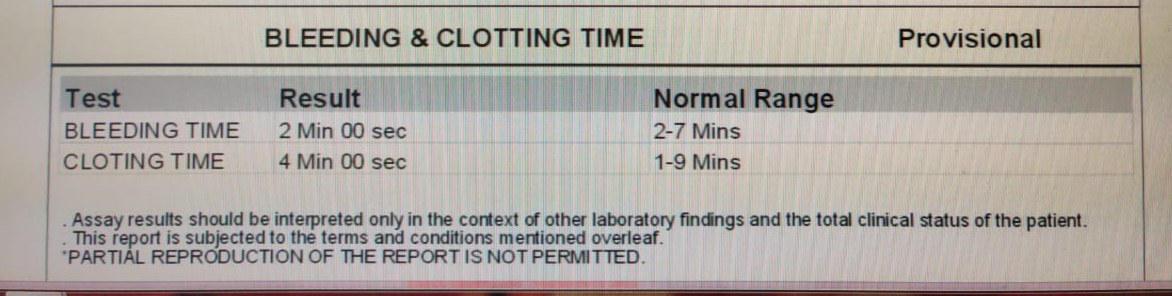
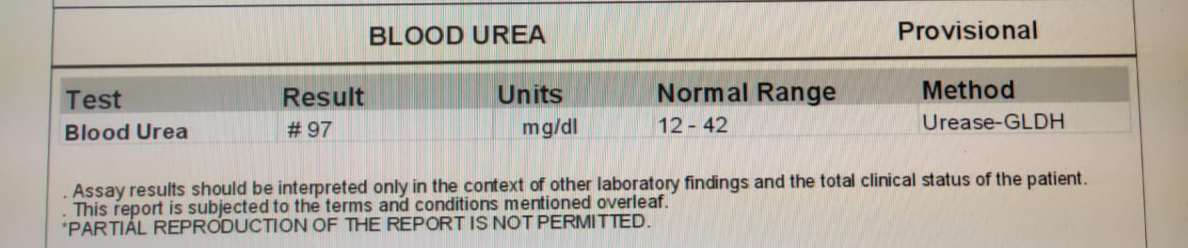
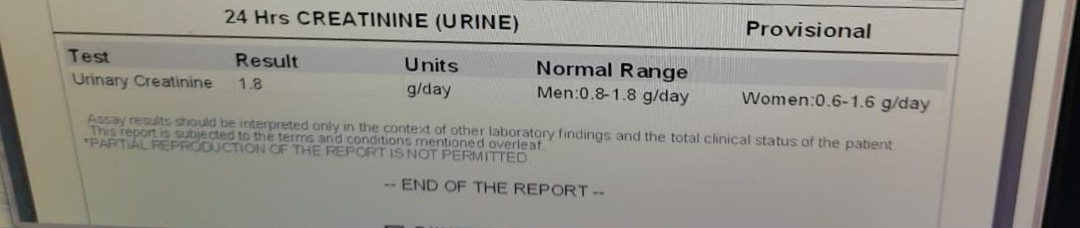
Investigations:-
1/6/23





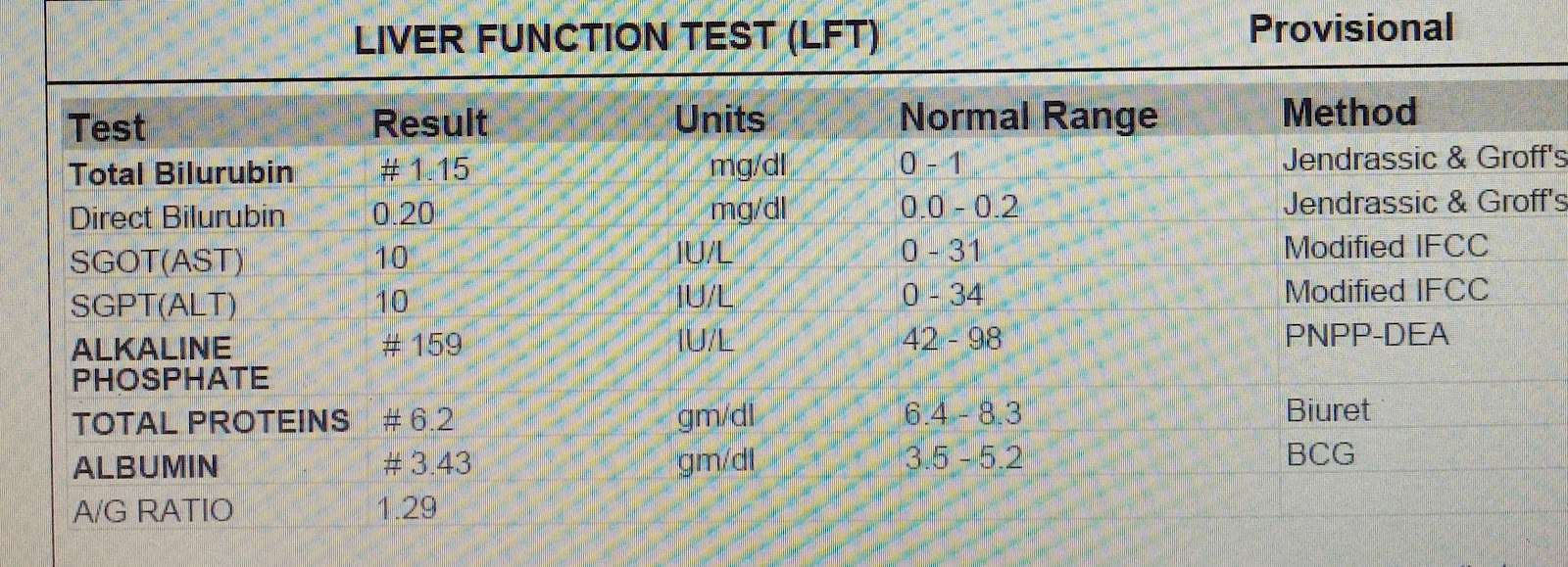















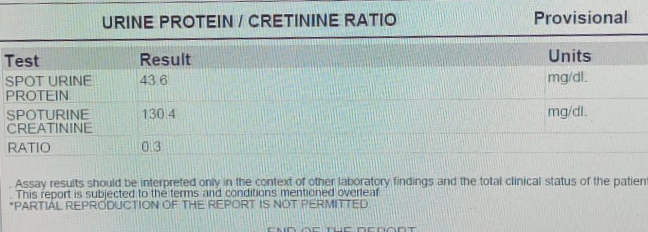






5/6/23






 Provisional diagnosis:-
Provisional diagnosis:-


Comments
Post a Comment